

A novel strain of coronavirus — SARS-CoV-2 — was first detected in December 2019 in Wuhan, a city in China’s Hubei province with a population of 11 million, after an outbreak of pneumonia without an obvious cause. The virus has now spread to over 200 countries and territories across the globe, and was characterised as a pandemic by the World Health Organization (WHO) on 11 March 2020.
As of 10 January 2021, there were 88,828,387 laboratory-confirmed cases of coronavirus disease 2019 (COVID-19) infection globally, with 1,926,625 reported deaths. The number of cases and deaths outside of China overtook those within the country on 16 March 2020.
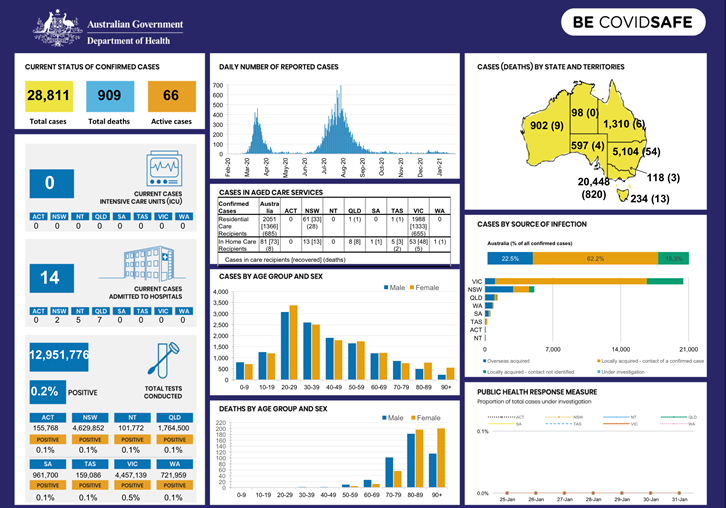
As of 31st January 2021, there have been 28811 confirmed cases of the virus in Australia and 909 of these have died. Infographic below from Department of Health indicated situation in various states and also other trends.
What are coronaviruses?
SARS-CoV-2 belongs to a family of single-stranded RNA viruses known as coronaviridae, a common type of virus which affects mammals, birds and reptiles.
In humans, it commonly causes mild infections, similar to the common cold, and accounts for 10–30% of upper respiratory tract infections in adults[4]. More serious infections are rare, although coronaviruses can cause enteric and neurological disease. The incubation period of a coronavirus varies but is generally up to two weeks.
Previous coronavirus outbreaks include Middle East respiratory syndrome (MERS), first reported in Saudi Arabia in September 2012, and severe acute respiratory syndrome (SARS), identified in southern China in 2003. MERS infected around 2,500 people and led to more than 850 deaths while SARS infected more than 8,000 people and resulted in nearly 800 deaths. The case fatality rates for these conditions were 35% and 10%, respectively.
SARS-CoV-2 is a new strain of coronavirus that has not been previously identified in humans. Although the incubation period of this strain is currently unknown, the United States Centers for Disease Control and Prevention indicate that symptoms may appear in as few as 2 days or as long as 14 days after exposure[6]. Chinese researchers have indicated that SARS-CoV-2 may be infectious during its incubation period.
The number of cases and deaths outside of China overtook those within it on 16 March 2020
Where has the new coronavirus come from?
It is currently unclear where the virus has come from. Originally, the virus was understood to have originated in a food market in Wuhan and subsequently spread from animal to human. Some research has claimed that the cross-species transmission may be between snake and human; however, this claim has been contested.
Mammals such as camels and bats have been implicated in previous coronavirus outbreaks, but it is not yet clear the exact animal origin, if any, of SARS-CoV-2.
How contagious is COVID-19?
Increasing numbers of confirmed diagnoses, including in healthcare professionals, has indicated that person-to-person spread of SARS-CoV-2 is common and each infected individual could infect between 1.4 and 2.5 people.
Similarly to other common respiratory tract infections, MERS and SARS are spread by respiratory droplets produced by an infected person when they sneeze or cough. Measures to guard against the infection work under the current assumption that SARS-CoV-2 is spread in the same manner.
How is COVID-19 diagnosed?
As this coronavirus affects the respiratory tract, common presenting symptoms include fever and dry cough, with some patients presenting with respiratory symptoms (e.g. sore throat, nasal congestion, malaise, headache and myalgia) or even struggling for breath.
In severe cases, the coronavirus can cause pneumonia, severe acute respiratory syndrome, kidney failure and death.
The case definition for COVID-19 is based on symptoms regardless of travel history or contact with confirmed cases. Diagnosis is suspected in patients with a new, continuous cough, fever or a loss or changed sense of normal smell or taste (anosmia). A diagnostic test is required in all suspected cases, and Australia has been quarantining suspected cases.
Who qualifies as a suspected COVID-19 case?
• fever
• dry cough
Other symptoms can include:
• shortness of breath
• sputum production
• fatigue
• sore throat
• loss of taste
• loss of smell
• diarrhoea
• nausea or vomiting
Less common symptoms include:
• headache
• myalgia/arthralgia
• chills
• nasal congestion
• haemoptysis
• conjunctival congestion
Older people may also have the following symptoms:
• increased confusion
• worsening chronic conditions of the lungs
• loss of appetite
Timeline of Covid 19 containment strategies in Australia
In March 2020, Australian government announced economic stimulus packages, closed international borders and implemented lockdown restrictions.
As the”curve flattened”, restrictions were eased in May 2020 but then reinstated in Victoria from June to October 2020.
31 December 2020
By this date, Australia recorded a total of 28,381 COVID cases and 909 deaths. The most affected state was Victoria, with 20,365 cases and 820 deaths, followed by NSW with 4,906 cases and 54 deaths, Queensland with 1,250 cases and 6 deaths, Western Australia with 859 cases and 9 deaths, South Australia with 575 cases and 4 deaths, the Australian Capital Territory with 118 cases and 3 deaths and the Northern Territory with 74 cases and 0 deaths.
The global tally reached 81, 475,053 confirmed COVID cases and 1,798,050 deaths reported to the WHO. The USA had the most confirmed cases (19,346,790), followed by India (10,266,674) and Brazil (7,563,551)
Australia’s response to Covid 19
Australia’s five-phase response to the pandemic included containment, reassurance amid uncertainty, cautious incrementalism, escalated national action and transition to a new normal.
Phase 1: Containment- mainly focussed on screening arrivals, quarantining vulnerable Australians and closing international borders.
Phase 2: Reassurance amid uncertainty- as number of cases remained low, health facilities were enhanced in preparation for increased demand.
Phase 3: Cautious incrementalism- self isolation of international arrivals, economic stimulus package and increased testing.
Phase 4: Escalated national action
As the number of cases began to increase, measures such as social distancing, canceling of elective surgery and progressive lockdown, school closures, increased testing, free childcare, increased economic support, and closure of interstate borders were initiated.
Phase 5: Transition to a new normal: measures such as social distancing, wearing of masks, contact tracing, ongoing requirements for testing, isolation, and quarantine.
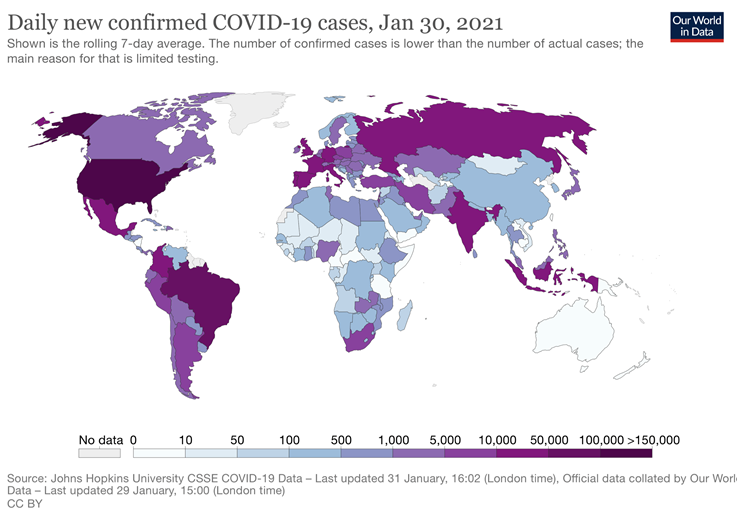
The below infographic is from John Hopkins University and demonstrates quite clearly how effective Australia has been successful in containing Covid.
Testing for COVID-19
The following groups are prioritised for testing:
- All people present with fever or acute respiratory illness (ARI). This represents the most important group on which to focus and increase testing.
- Contacts of cases.
- Asymptomatic testing in outbreak settings. There may be other circumstances where clinical and public health judgment lead to a decision to conduct asymptomatic testing. These groups include:
- People at risk of exposure who present with atypical symptoms.
- At-risk populations and settings where time-limited testing is used to provide an upper estimate of transmission in these groups or settings.
Economic stimulus package/ tax relief measures
- Tax-free withdrawals from superannuation funds.
- Tax-free payments made to certain employers (to support small and medium-sized businesses)
- Tax depreciation write-off
- Businesses can claim an immediate deduction for multiple assets, new or second-hand, provided each asset costs less than AU$150,000
- Tasmania announced a waiver of payroll tax for the last four months of 2020
- New South Wales announced AU$450 million for the waiver of payroll tax for businesses
- Queensland businesses affected by the coronavirus outbreak can defer their payroll tax payment for six months
- Victoria- businesses with annual taxable wages up to $3 million had payroll tax for the 2019-20 financial year waived.
- Jobkeeper package to support businesses who suffered the loss of income due to COVID
- Jobseeker package
- Landlord land tax relief
- Rent deferral and rent relief
Medications – any concerns with COVID –19?
Concerns raised over use of medications for blood pressure (ACE inhibitors) and anti inflammatories (Ibuprofen) were investigated- no clear evidence that any of these should be avoided.
Guidelines for managing COVID-19 patients:
Many international resources are available – including WHO, National Institute of Health, CDC in the US, NICE (National Institute for Health and Care Excellence, UK) guidelines on clinical management, treatment and use of experimental therapies. There are national guidelines developed by National Covid-19 Clinical Evidence Taskforce.
Did the coronavirus cause any medicines shortages?
Anticipated shortages of chloroquine, azithromycin, dexamethasone, paracetamol and morphine, was managed by preventing parallel export of these medications. These were all tested as possible treatments for COVID 19. A further 150 medications, used in anaesthesia, intensive care and emergency were also banned from export. This preempted any serious drug shortages.
Are there drugs to treat COVID-19?
Information about COVID has evolved so quickly that it can be difficult for clinicians to feel confident that they are staying current.
While treatment for COVID-19 outside of the hospital setting is currently limited to supportive therapy, over 1000 clinical trials are underway looking at a range of drug treatments. Here is a quick summary of the current state of evidence.
Remdesivir
Bottom line on remdesivir. Remdesivir is administered intravenously, limiting its use to hospitalized patients. However, phase 1 trials of an inhaled nebulized version were initiated in late June 2020 to determine whether remdesivir can be used on an outpatient basis and at earlier stages of disease.
Dexamethasone
Bottom line on dexamethasone. While steroids are not generally recommended for treatment of COVID-19 or any viral pneumonia, the UK RECOVERY trial changed that. IDSA guidelines include low-dose dexamethasone (6 mg orally or intravenously daily for 10 days) in patients requiring respiratory support. At present, the World Health Organization has cautioned clinicians to reserve use for severely ill patients.
Hydroxychloroquine (HCQ)
Bottom line on HCQ. While some continue to tout its benefit, particularly if given early in the course of infection, there is little evidence at this time to support its use at any stage of illness.
Other Antimicrobials
In the race to find an effective therapy, clinicians around the world have launched trials of a wide range of agents, with almost universally disappointing results.
Azithromycin: While some initial trials of azithromycin in combination with HCQ were promising, later results have not held up and major cardiology organizations now warn against the combination. There are no recommendations for use of this antimicrobial.
A Grab Bag of Other Drugs
- Convalescent plasma.
- Colchicine.
- Nitric oxide.
- Zinc.
- Monoclonal antibodies.
Summary:
- Since coronavirus disease 2019 (COVID‐19) emerged in Wuhan, China in December 2019 and spread around the world, over 3500 clinical studies have been registered as per WHO database.
- Such rapid development and launch of clinical trials is impressive but presents challenges, including the potential for duplication and competition.
- There is currently no known effective treatment for COVID‐19.
Is there a vaccine and how do vaccines work?
There are hundreds of Covid-19 vaccines in development, and some have produced very positive results in phase III clinical trials. Some countries including USA, UK, India, Brazil and china have vaccinated millions of people and are continuing this on a war footing.
All vaccines work by teaching our bodies to recognise and fight the pathogen in a safe way. They encourage our immune system to produce antibodies, T-cells or both, so that if we encounter the infection later our immune system knows how to defend against it.
Viral vector vaccines
A harmless virus is altered by introducing part of the disease-causing virus’ genetic code, such as the code for Covid-19’s ‘spike’ protein.
The harmless virus transports the code into our cells – in a similar way to RNA vaccines – which then start to produce the protein.
This triggers an immune response, priming our immune system to attack the real virus later.
Oxford-AstraZeneca is the first viral vector vaccine to be approved for Covid-19. More are in late-stage research, such as CanSino Biologics, Gamaleya Research Institute and Janssen. They all use adenoviruses – a group of viruses that cause the common cold – as the vector or carrier.
Another example of a viral vector vaccine is the Ervebo (rVSV-ZEBOV) Ebola vaccine – it uses the vesicular stomatitis virus as the carrier.
RNA vaccines
Messenger RNA is a sequence of genetic code which our bodies use all the time – it tells our cells what proteins to build so they can function.
To produce an RNA vaccine, scientists develop a synthetic version of the virus’ messenger RNA.
When this is injected into our bodies, cells read it as an instruction to start building the relevant viral protein, for example Covid-19’s ‘spike’ protein. This prompts our immune system to respond, and in doing so it learns how to protect against future Covid-19 infection.
Two RNA Covid-19 vaccines have been approved for use: Pfizer-BioNTech and Moderna. Both have reported high levels of vaccine efficacy – around 95%.
They are the first RNA vaccines ever to be approved for use against any disease. However, researchers have been using the technology for a while, and people have been given RNA vaccines in clinical trials for other diseases, like cancer.
‘Whole’ virus vaccines
These vaccines could be:
Inactivated – a version of the virus is inactivated by being exposed to heat, chemicals or radiation.
Virus-like particle – a version of the virus, closely resembling the real thing, is created artificially, however it doesn’t contain any genetic material, so it’s not infectious.
These vaccines cannot cause the disease, but will cause our bodies to produce an immune response which will protect against future infection.
Some of the most advanced inactivated Covid-19 vaccines in development include Sinovac, Bharat Biotech and two by Sinopharm. Examples of existing inactivated vaccines include the whooping cough, rabies and hepatitis A vaccines.
One vaccine in phase III clinical trials is virus-like particle: Medicago Inc. An example of an existing vaccine is the HPV/cervical cancer vaccine.
Protein subunit vaccines
A small piece of the virus’ genetic code is inserted into another cell – perhaps a bacterial, yeast, mammalian or insect cell. The code contains instructions for this cell to start building the virus protein, for example the Covid-19 ‘spike’ protein.
Cells like this act as factories, building large quantities of the protein – which is then extracted, purified and used as the active ingredient in the vaccine.
When it is injected, our bodies learn to recognise the viral protein so that they can mount an immune response which protects against future infection.
Some of the most advanced Covid-19 vaccines using this approach include Novavax and Chinese Academy of Sciences.
An example of an existing protein subunit vaccine is for hepatitis B, which uses yeast cells to build the virus protein.
How do the different Covid-19 vaccines compare?
The different vaccine approaches present different opportunities and challenges, which is why we’ll need a range of vaccines to get control of the pandemic.
The containment of this pandemic depends on worldwide control, through vaccines that need to be made affordable and accessible to all countries.
Low-income countries may face challenges of procurement, storage, and distribution of vaccine- equitable access needs to be ensured.
Summary of available vaccines types:
| Technology/ company | Suitable for those with low immunity | Number of doses | Storage | Other vaccines with this technology |
| RNA Pfizer Moderna | YES | 2 | Pfizer : -70 deg C Moderna: -20deg C | NIL |
| VIRAL VECTOR Astra Zeneca CanSino Janssen Gamalaya | YES | 1-2 | 2-8 degC | Ebola |
| WHOLE VIRUS- INACTIVATED Sinovac Bharat Biotech Sinopharm | YES | 2 | 2-8 degC | Whooping cough/ Rabies/ Hep A/ HPV- cervical cancer |
| PROTEIN SUBUNIT Novavax Chinese academy | YES | 2 | 2-8 deg C | Hep B |
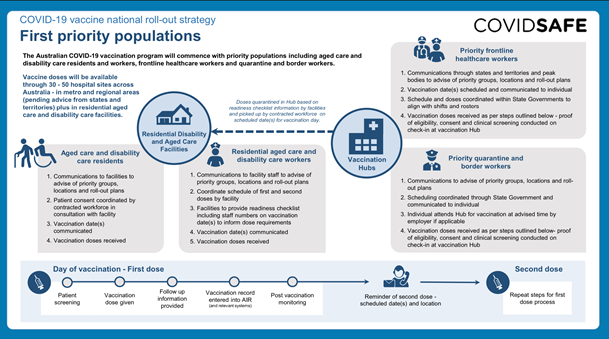
Covid-19 vaccine National roll-out strategy
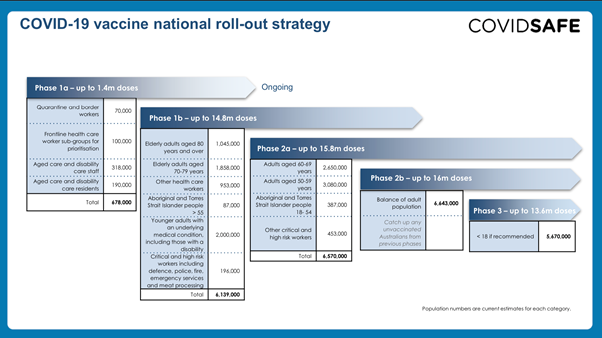
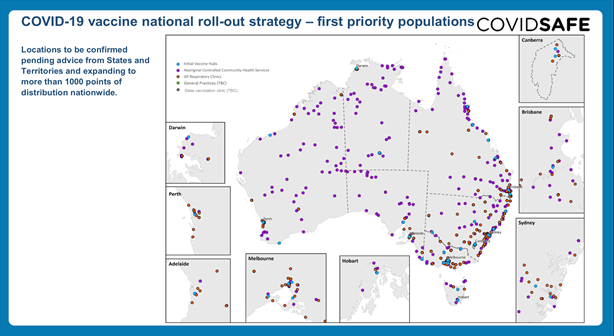
Whilst we await results of vaccination, it is currently being undertaken worldwide as the major hope of containing this infectious viral pandemic.
This article is written by:
Dr. Sanjay Sharma
Consultant Anaesthetic

Dr. Deepika Monga
Consultant Obstetrian and Gynecology
